In 2026, clinicians will confront a paradox within the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA), bipartisan legislation the American Medical Association once hailed as ending an “era of uncertainty” for physician reimbursement. The paradox stems from divergence in annual updates to the Medicare conversion factor — the dollar amount that translates the relative value units (RVUs) assigned to medical services into actual Medicare payment rates.
Beginning in 2026, clinicians who qualify through Advanced Alternative Payment Models (APMs), a category of value-based models defined under MACRA, will receive a 0.75% annual update to the conversion factor, while all others will see only a 0.25% increase. Over time, these updates will compound, creating a structural advantage for Qualifying APM Participants (QPs). In the short term, however, high-performing clinicians who remain in the Merit-based Incentive Payment System (MIPS) may earn larger gains through performance-based payment adjustments than through the relatively modest conversion factor differential.
(Analysis by Katie Lawler)
MACRA was established to replace a flawed predecessor. Before 2015, physician payments were tied to the Sustainable Growth Rate (SGR) formula, which automatically reduced payment rates whenever Medicare spending exceeded set targets. Because healthcare costs regularly outpaced those targets, the SGR called for deep, across-the-board cuts year after year — reductions that were widely considered untenable. To prevent disruption in physician participation, Congress intervened 17 times with temporary fixes, known as the “doc fix,” to override the scheduled cuts. By 2015, a 21% reduction loomed unless Congress acted again.
MACRA was intended as a permanent remedy. It repealed the SGR, set stable conversion factor updates between 0% and 0.5% for 2015 through 2024, and created the Quality Payment Program (QPP) to link future payment updates more directly to value.
The QPP established two tracks: one for Qualifying APM Participants (QPs) and one for everyone else, referred to here as non-QPs.[1] Each track is governed by its own rules, incentives, and — beginning in 2026 — separate conversion factor updates.
First Track – Qualifying Participants (QPs)
The first track is for Qualifying APM Participants (QPs) in Advanced APMs[2]. QPs are those who move a substantial portion of their practice through an Advanced APM — 75% of payments or 50% of patients—and are then categorically excluded from MIPS. QP status applies to an eligible clinician’s National Provider Identification (NPI) under all Taxpayer Identification Numbers (TINs) through which they bill.
In the introductory years of the program, QPs received a 5% lump sum “QP Incentive Payment” on all Part B claims submitted to CMS during the base year. This 5% Incentive Payment was extended, and then reduced and extended further as Congress was pressured to continue to extend the windfall. However, beginning in payment year 2026, the Incentive Payments will finally be replaced by the statutorily mandated enhanced QP conversion factor update.
Second Track – Non-QPs
Clinicians who are not QPs are in the “non-QP” track of the QPP. Those who meet certain criteria, such as exceeding a minimum Part B billing threshold, are required to participate in MIPS at the TIN/NPI level. Based on their performance across four performance categories — quality, improvement activities, cost, and Promoting Interoperability — MIPS-eligible clinicians receive a composite MIPS performance score. A budget-neutral MIPS payment adjustment is then calculated for each MIPS-eligible clinician and applied to subsequent Part B claims submitted under that TIN/NPI.
MIPS adjustments maintain budget neutrality by applying performance-based negative payment adjustments to clinicians below the MIPS performance threshold and using that money to fund scaled, upward adjustments for those above the threshold. While there is no cap on potential upward adjustments, downward adjustments may not exceed –9%.
A simplified example illustrates how this works: in a year when 50% of clinicians failed to report and earned a 0% performance score, those clinicians would receive the maximum negative adjustment of –9%. If the remaining 50% of clinicians earned perfect scores and billed for roughly the same volume of claims as those with negative adjustments, those with perfect scores would see an upward adjustment of +9%. If those earning above the benchmark had more stratified scores — for example, 25% of all clinicians earned a score only slightly above the benchmark and 25% earned perfect scores — the MIPS adjustment for those near the benchmark would be closer to +1%, while the high performers might earn +8%. The difference in payment reflects performance relative to peers while keeping the program budget-neutral.
In the early years of the program, the performance threshold was relatively low, and COVID hardship exceptions were readily available. As a result, the proportion of clinicians falling below the performance threshold was small, and upward adjustments were modest, typically ranging from +0.2% to +2.1%.
Statutory requirements have since forced the performance threshold significantly higher — from 25% in the first year to 75% in 2025 — and it may continue to rise, though at a slower pace. This will likely result in more participants falling below the performance threshold, making more money available for upward adjustments for high performers in MIPS.
Conversion Factor Updates
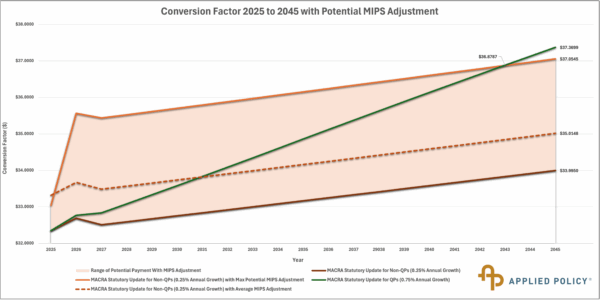
Beginning in 2026, the two tracks of the QPP will see their conversion factors diverge for the first time. QPs will receive an annual update of +0.75%, which will compound annually. Non-QPs will receive a +0.25% annual update, which will also compound annually.
This rate of compounding means that the conversion factor for QPs will grow more quickly than the conversion factor for non-QPs, and the difference between them will eventually be substantial. In the short term, however, the relatively small difference in conversion factor updates — combined with the potential for larger upward MIPS adjustments available to high performers — could mean that for several years, MIPS, rather than QP status, remains the more financially profitable track of the QPP.
Conclusion
MACRA resolved one longstanding problem by repealing the SGR and ending the cycle of annual “doc fixes.” But in doing so, it created a new tension: two tracks within the QPP now point clinicians in different directions. The MIPS track offers annual adjustments that can be meaningful in the near term, while the QP track advances more gradually, embedding higher updates into the conversion factor over time. This paradox of short-term incentives working against long-term policy goals underscores the complexity of aligning Medicare payment reform with the broader shift toward value-based care.
[1] This is confusingly referred to as the “non-APM” track by CMS in some documents, but it is important to remember that most APM participants are not QPs, and a large plurality of clinicians in the “non-APM track” are, in fact, in APMs. For clarity, we refer to this track as “non-QP”.
[2] APMs that require sufficient downside financial risk, quality measures tied to payment, and use of Certified EHR Technology (CEHRT).