How sustainable is Medicare physician payment under current law?
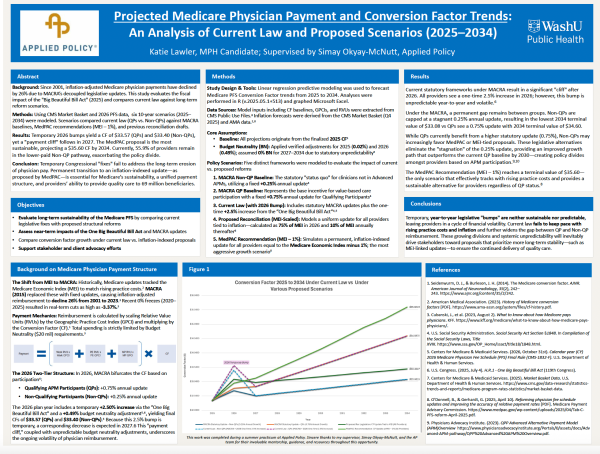
The answer to this question has significant implications for physician reimbursement, practice sustainability, and the nearly 69 million beneficiaries covered by Medicare. It also served as the foundation for a recent practicum project conducted at Applied Policy examining Medicare Physician Fee Schedule conversion factor trends under current law and several proposed reform scenarios through 2034.
Completed by Katie Lawler in collaboration with Senior Health Policy Manager Simay Okyay McNutt, the project drew on Centers for Medicare & Medicaid Services (CMS) data, long-range modeling, and policy analysis to examine how different update structures could shape physician reimbursement over the coming decade.
Lawler modeled six payment scenarios from 2025 through 2034, comparing current law against several proposed reform approaches, including inflation-linked updates and recommendations from the Medicare Payment Advisory Commission (MedPAC). Among the findings was a projected “payment cliff” following temporary 2026 increases, as well as continued divergence between qualifying alternative payment model participants and other providers under the Medicare Access and CHIP Reauthorization Act (MACRA).
In presenting her findings at Washington University in St. Louis in May, Lawler noted that under current law, neither Alternative Payment Models (APMs) nor non-APM payment pathways keep pace with rising practice costs. “Although the temporary ‘bump’ helps, it won’t keep pace with inflation down the line and is not guaranteed year-to-year.”
The analysis also revealed a growing payment gap between the two provider groups — with non-APM providers facing a terminal conversion factor of $33.08 by 2034 compared to approximately $34.60 for APM participants — a divide that may increasingly fragment how different provider groups advocate for payment reform.
From Internship to Professional Development
Okyay McNutt observed that the value of the research extended beyond its findings.
“As Katie moved through the project, I saw her develop a deeper appreciation for how the quality and precision of healthcare data shape our understanding of the financial pressures providers face,” Okyay McNutt said. “Far from being purely academic or theoretical, such work helps stakeholders better understand how policy decisions may affect healthcare delivery over time.”
This practical exposure to health policy analysis was exactly what Lawler hoped to gain when she first emailed Applied Policy COO John Voorhees in 2024 to inquire about a summer internship.
“Katie was preparing to start her master’s studies through Washington University’s accelerated ‘3-2’ program,” said Voorhees. “From the beginning, she was interested in pairing academic work with practical policy experience, particularly related to CMS and the federal policymaking process. Like many of our interns, she was drawn to the opportunity to have a real seat at the table in Washington policy conversations.”
Following Policy Debates
Many of Lawler’s early assignments as an intern involved tracking MedPAC discussions and congressional activity, including hearings and policy proposals emerging from the House Ways and Means Committee and Senate Finance Committee.
Among the issues drawing increasing attention was the divergence in Medicare physician payment updates scheduled to take effect under MACRA. Beginning in 2026, clinicians participating in qualifying advanced alternative payment models will receive annual conversion factor updates of 0.75%, while other clinicians will receive annual updates of 0.25%, creating a two-tier payment structure within the Physician Fee Schedule.
After completing her initial summer internship, Lawler continued working remotely with Applied Policy while further developing her quantitative and analytical skills through graduate studies in biostatistics and epidemiology. She remained focused on the long-term implications of different payment approaches, including how inflation, temporary legislative increases, and diverging update pathways under MACRA could affect reimbursement stability.
A central premise of the project was that modest annual differences can produce substantially different outcomes when compounded over many years. Understanding those long-term effects required looking beyond individual payment updates and modeling how different policy approaches would perform over time.
“Listening to discussions on Capitol Hill and hearing the concerns of Applied Policy’s health services clients made me want to understand what these numbers would actually mean over time,” said Lawler. “It’s one thing to say that a payment rate is increasing by a fraction of a percent. It’s another to understand what that means for a physician’s practice a decade later.”
Modeling Outcomes
When Lawler expressed an interest in pursuing the topic as a practicum project, Voorhees saw a natural fit in Okyay McNutt as a mentor. Okyay McNutt’s own career at Applied Policy had begun as an intern, and her experience in physician reimbursement policy and healthcare data analysis made her uniquely positioned to help guide the project.
Okyay McNutt helped Lawler translate her questions into a research framework, emphasizing the importance of modeling multiple scenarios to reflect the range of physician payment approaches under discussion in Washington and the uncertainty surrounding future reimbursement policy.
The final model incorporated current-law payment updates, alternative approaches tied to inflation, recommendations from MedPAC, and physician payment proposals emerging from congressional negotiations. Several scenarios reflected proposals actively under consideration in Congress, while others were designed to test how inflation-linked updates and alternative policy frameworks would perform over time.
By examining multiple possible pathways side by side, the project sought to illustrate how seemingly small differences in annual updates can compound over time. As congressional negotiations progressed, the model was expanded to incorporate physician payment proposals contained in multiple versions of the “One Big Beautiful Bill Act” debated during the spring of 2025.
“Part of working in health policy is understanding that the landscape rarely stands still,” said Okyay McNutt. “As different versions of legislation emerge and negotiations continue, analysts have to revisit assumptions, update models, and reassess how policy changes may affect stakeholders over time.”
Discussing her findings, Lawler characterized the current Medicare physician payment system as “a volatile cycle of temporary legislative fixes that fail to account for inflation, creating a widening gap between provider reimbursement and the actual cost of delivering quality care.” She observed that this has direct implications for the beneficiaries who depend on the physicians those payments are meant to sustain.
While Lawler’s experience was unique in that it culminated in a graduate-level practicum, it reflects the kind of substantive policy work Applied Policy interns are supported in pursuing. As Voorhees observes, the Applied Policy internship program has always been built around one principle: that rising health policy professionals should be presented with the opportunity to engage in consequential policy analysis from the start.
Download a copy of Lawler’s presentation poster below.